(download as a pdf - 7.4Mb)
The purpose of wound cleaning is to remove debris from the wound and surrounding skin to minimize the impact of that debris on healing. There are some general principles that can be applied to all situations, however each wound needs to be assessed individually to create a suitable wound cleaning plan. For example, a skin tear that was cleaned, edges re-opposed and dressed 2 days ago. You lift the edge of the silicone dressing and there is no exudate, the skin is clean, dry and pink. Do you clean it? I would not. The risk of disturbing the delicate skin out-weighs the benefit of cleaning. What about the arterial heel or toe wound? The person has no ability to heel this (or very limited). Do you clean it? If it is dry necrotic material I would really hesitate to get it wet. What about the fungating tumour? High risk of bleeding but countering that is the high risk of infection … it is about assessing the risks and working out a plan with the treatment team, the patient and their family/carer that is best for the patient.
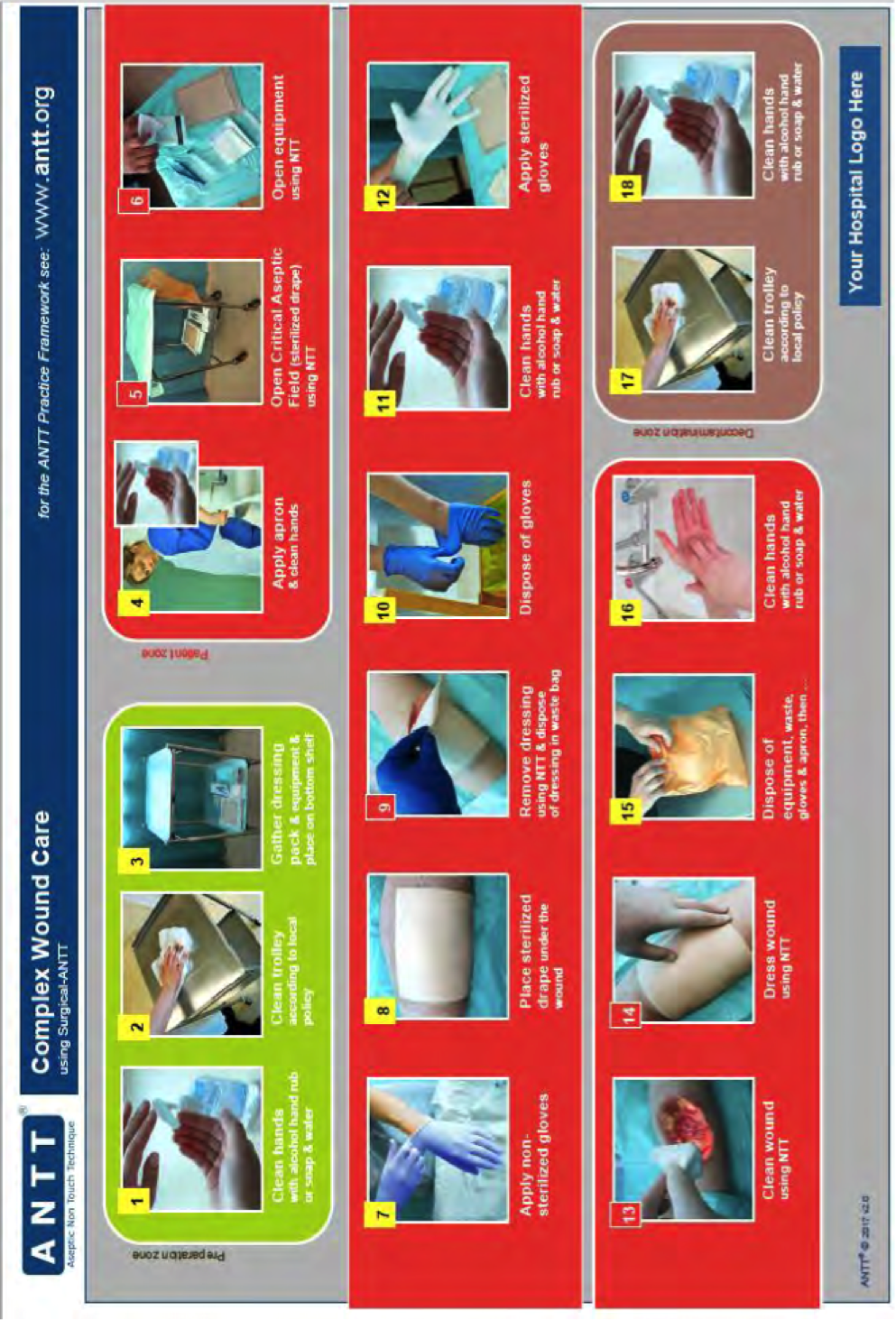
Generally speaking, there are a number of things to do to minimize infection when interacting with a wound. Most recently the aseptic non-touch technique (ANTT) has been promoted as current best practice. Some key points(2) are:
A copy of the ANTT can be seen in Appendix A.
Gloves: sterile, non-sterile or none? The only place (in my opinion) you could possible not wear gloves is when setting up the field. This assumes you have washed your hands thoroughly before-hand. But I tend to wear gloves for this as well. When interacting with the skin and the wound, this is a judgment call. A systematic review of cutaneous and dental surgical procedures showed no significant difference between using clean or sterile gloves (3). However, assess the individual and the situation. Are they at higher risk for infection? Are you reaching into a body cavity? Is bone or are other internal structures exposed?
Potable tap water. This is water that has been deemed suitable for drinking. Potable tap water can be used on adults and children with acute or chornic wounds(4). If potable water is not available boiled and cooled water is an acceptable substitute(2). Potable water has been shown to be cost effective, readily available and not cause harm or increase the risk of infection in these wounds(5). However, by itself, it is also not able to interrupt biofilm and pseudomonas aeruginosa is known to colonise wet areas (taps and pipes)(6).
Normal saline. This is available as a 0.9% solution of sodium chloride in water. This may be needed for patients where potable water is deemed unsuitable. Normal saline has been shown to not harm healing wound tissues. However is has no effect on biofilm(1) and bacterial growth can occur in an open container within 24 hours(6).

Prontosan. This is a solution of 0.1% Polyhexamethylene biguanide (PHMB), an antimicrobial agent and 0.1% Betaine, a surfactant. Hypersensitivity is rare but possible so should only be used on patients who have not shown a previous sensitivity to the product(2). The solution’s surfactant component has been shown to penetrate difficult to remove coating, breaking up biofilm and suspending it in solution to prevent re-contamination(6). In order for the antimicrobial component to be effect the product must be in contact with the wound for at least 15 minutes(5). PHMB’s mechanism of action also means it has a low risk of developing resistances(7).
Povidone-Iodine. This has been known to show toxicity to healthy cells in high concentrations and longer duration of contact but has shown efficacy against biofilms with reduced concentrations (1%w/v available iodine) and 15-minute exposure time. It is recommended to rinse the product off after use(1). There have also been reports of renal and thyroid dysfunction where there have been large absorption sites and prolonged use(2).
Acetic Acid (Vinegar). There is very little in the modern literature that discusses the use of vinegar in wound cleansing. A 1% solution has been shown to reduce Pseudomonas aeruginosa colonization better than normal saline(8). It is not as effective against other bacteria(9). But as anyone who has ever had fish-n-chips with finger cuts or cracked lips can attest to, at higher concentrations this stuff can really burn! Therefore preparation needs to be precise and calculating exactly how much of the particular vinegar you have that you need to make a 1% solution is adding in a possible step for mistakes.
Potassium Permanganate (Condies Crystals). Again, there is little research supporting the use of Potassium Permanganate in wound management but anecdotally it has been used to manage weeping or blistering conditions such as acute weeping/infected eczema and leg ulcers. However the NHS commissioned a study (“What is the evidence for the use of potassium permanganate preparations?”) in 2019 that found no statistically significant support for it’s use. DermNet NZ describes it’s use in “wet” skin conditions at a dilution of 1 in 10,000 and as a 1% (1 in a 100) solution when managing fungal infections such as athlete's foot(10). But at higher concentrations the solution is caustic and can burn the skin. It can also cause irritations at lower concentrations with repeated use.

Image source from DermnetNZ
Hydrogen Peroxide. H2O2 is a naturally occurring chemical in the body that has a great influence on wound healing. The concentrations of H2O2 change throughout the different stages of wound healing, changing it’s role at each stage. In high concentrations it is pro-inflammatory and at low concentrations it promotes the secretion of cytokines that help with tissue regeneration(11). We don’t really know how exogenous sources of H2O2 impact on wound healing, but it still appears widely used in surgical procedures, particularly in the UK. However, it’s efficacy is questionable and it is known to have reduced antimicrobial efficacy in the presence of organic matter (such as proteins/blood)(12). It is also known to be cytotoxic, to the extent that it was once recommended as a form of cancer treatment for killing solid tumours(13).
Hypochlorus Acid. This appears to be gaining momentum again in the wound world despite it being quite cytotoxic. However the version used in wound cleansing is around 0.01% and is considered safe to use with rapid and broad antimicrobial efficacy(6). It is also thought to impact on biofilms(14). A 15 minute exposure is said to be effective against gram negative bacteria and can also help to facilitate the separation of non-viable tissues(1).
Chlorhexidine. Resistances to Chlorhexidine have now been found in Proteus Mirabilis, Pseudomonas sp. and S. Aureus. In rare cases it can also cause anaphylaxis(2). Chlorhexidine comes in different concentrations and formulations for different applications such as skin preparation and wound irrigation. However the wound irrigation concentrations have not been found to increase wound healing rates and other, safer, solutions should be considered(15).
Showering. Shower pressure is sufficient to dislodge surface debris and can be used in conjunction with disposable washcloths to provide additional mechanical force. Showering may also give patients a feeling of well-being and cleanliness. Consideration needs to be given to the quality of the water and the possibility of bacterial contamination of the shower, taps and pipes.
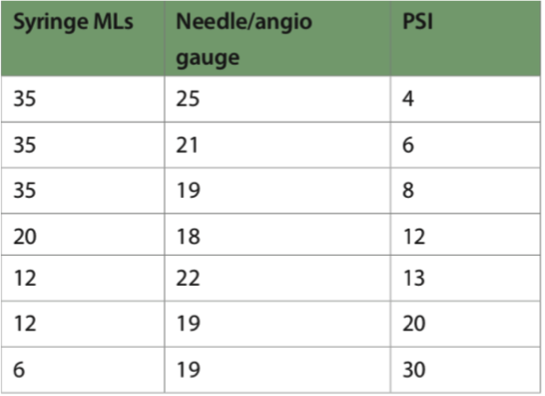
Irrigation. 15 PSI of pressure is achievable by using a 20ml syringe with a 20g cannula. This level of pressure has been shown to dislodge bacteria on the wound. Lower pressures can be used to provide wound cleaning for granulating tissues(1). The use of sterile gauze squares may provide additional mechanical force if needed.
Soaking. Soaking is used where surfactants are involved and it allows the product time to break up the biofilm. Irrigate the wound first to remove loose debris, then apply the solution to a sterile gauze and place in the wound bed. Leave in place for 15 minutes(5). The wound may also be cleaned with soaked sterile gauze squares to provide additional mechanical force if needed.
Cellular activity decreases with decreasing temperature. This means that every time we interact with a wound (expose it to air, wash it, leave it uncovered awaiting doctor review or community nurse visit …) we slow down the healing. Warming solutions and keeping wounds covered/not disturbed as long as possible assist to keep the cellular activity unimpeded(1). Ensure that you read the instructions on the solutions you are using as some may be more irritating if warmed or may reduce their shelf-life.
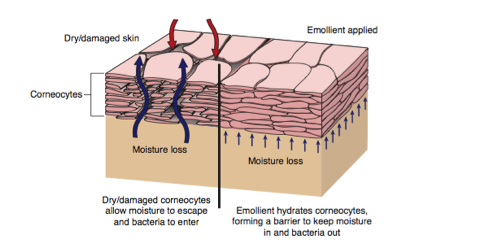
An emollient is an oil suspended in an emulsion that will put an occlusive coating on the skin(16). The purpose of emollients is to improve the moisture retaining capability of the skin. The barrier function of the skin relies on a well-hydrated epidermis. It is also this level of moisture in the stratum corneum that helps to regulate the pliability and elasticity of the skin(17).
The degree to which the emollient traps moisture to the skin varies with the composition of the product. Generally speaking moisture retention increases with density: Oils < Lotions < Creams < Ointments(16, 18).
The use of emollients is most effective after bathing(16) and it is recommended that they be applied in the direction of the hair follicles and as often as needed to keep the skin well hydrated(18).
There can be adverse effects related to the use of emollients. Contact allergies are rare but may be related to something like a preservative or fragrance. Patch testing can be used on sensitive patients or if you have any concerns. The more highly occlusive emollients can cause or aggravate folliculitis. And the presence of paraffin-containing ointments on clothing or bedding can be a fire hazard if exposed to cigarettes or a lighted fire(16, 19). Where these products have spilled onto the floor it can also be a slip hazard(18).
Compression garments can be difficult to get on and difficult to get off. Lower leg ulcers occur more often in patients over 65 years of age and strength and dexterity in this age group will impact on the ability to put garments on or take them off. This is well known and there is a wide selection of devices that can assist with donning and doffing, a few of which are listed here.
| Image | Style | Benefits | Considerations |
|---|---|---|---|
 | Slider or slide sheet style |
|
|
 | Slider style with magnets (for closed toe garments) |
|
|
 | Plastic support frame |
|
|
 | Metal support frame |
|
|
 | Bubble |
|
|
 | Plastic frame with doffing aid |
|
|
 | Doffing aid | Assists in the removal of garments | Useful for removing lighter garments. Will eventually break with enough pressure or used on too much of an angle. At which point it becomes a potential skin damage risk. |
Appendix A(1) - ANTT for Simple Wounds (2.2Mb)

Appendix A(2) - ANTT for Complex Wounds (2.1Mb)
1. Weir, D. and T. Swanson, Ten top tips: wound cleansing. Wounds International, 2019. 10(4): p. 8-11.
2. Nolan, M., HSE National Wound Management Guidelines 2018, T.O.o.N.a.M.S. Director, Editor 2018: Dublin, Ireland.
3. Brewer, J.D., et al., Comparison of Sterile vs Nonsterile Gloves in Cutaneous Surgery and Common Outpatient Dental Procedures: A Systematic Review and Meta-analysis. JAMA Dermatology, 2016. 152(9): p. 1008-1014.
4. Fernandez, R. and R. Griffiths, Water for wound cleansing. Cochrane Database of Systematic Reviews, 2012(2).
5. Mahoney, K., Part 2: Wound cleansing and debridement. Journal of Community Nursing, 2020. 34(3): p. 26-32.
6. Wolcott, R. and J. Fletcher, The role of wound cleansing in the management of wounds. Wounds International, 2014. 5(3): p. 25-30.
7. Worsley, A., et al., Polyhexamethylene Biguanide:Polyurethane Blend Nanofibrous Membranes for Wound Infection Control. Polymers, 2019. 11(5): p. 915.
8. Madhusudhan, V.L., Efficacy of 1% acetic acid in the treatment of chronic wounds infected with Pseudomonas aeruginosa: prospective randomised controlled clinical trial. International Wound Journal, 2016. 13(6): p. 1129-1136.
9. Kumara, D.U.A., et al., Evaluation of bactericidal effect of three antiseptics on bacteria isolated from wounds. Journal of Wound Care, 2015. 24(1): p. 5-10.
10. "Potassium Permanganate". Dermnet NZ 2016 [cited 2016, September 4]; Available from: http://www.dermnetnz.org/topics/potassium-permanganate/.
11. Zhu, G., et al., Hydrogen Peroxide: A Potential Wound Therapeutic Target? Medical Principles & Practice, 2017. 26(4): p. 301-308.
12. Roth, B., et al., Effect of antiseptic irrigation on infection rates of traumatic soft tissue wounds: a longitudinal cohort study. Journal of wound care, 2017. 26(3): p. 79-87.
13. Symons, M.C.R., et al., Hydrogen peroxide: a potent cytotoxic agent effective in causing cellular damage and used in the possible treatment for certain tumours. Medical hypotheses, 2001. 57(1): p. 56-58.
14. International Wound Infection Institute, Wound Infection in Clinical Practice: Principles of Best Practice. Wounds International, 2016.
15. Wound Healing and Management Node Group, Evidence Summary: Wound management - Chlorhexidine. Wound Practice & Research, 2017. 25(1): p. 49-51.
16. "Emollients and moisturisers". Dermnet NZ 2016 [cited 2021, August 19]; Available from: https://dermnetnz.org/topics/emollients-and-moisturisers/.
17. Watkins, P., Using emollients to restore and maintain skin integrity. Nursing Standard, 2008. 22(41): p. 51-57.
18. Flavell, T., Using soap substitutes, bath additives and leave-on emollients. Journal of Community Nursing, 2016. 30(3): p. 29-34.
19. Penzer-Hick, R., Fire risks and skin creams: some history and an update. Journal of Community Nursing, 2020. 34(6): p. 14-14.
© 2015 Wound Care Resource All rights reserved | Web template modified from W3layouts